Introduction-
“The Mind can be its own cage.”
Imagine being Trapped in a Cycle of Unwanted Thoughts and Repetitive actions that you cannot control. For Someone with Obsessive–Compulsive Disorder (OCD), this is daily reality. OCD is not about being tidy or particular—it is a Chronic Psychiatric Disorder that disrupts Thinking, Emotions, and Behavior, often Leading to Significant Distress and Impairment.
According to the World Health Organization (2023), OCD is Among the Top 20 Disabling Illnesses Worldwide. In India, Studies Estimate the Lifetime Prevalence of OCD at about 0.6–3% of the population, affecting both Children and Adults.
Definition
OCD is defined as a Mental Health Disorder characterized by:
- Obsessions → Intrusive, Persistent, Unwanted Thoughts, Images, or Urges.
- Compulsions → Repetitive Behaviors or Mental Acts Performed to Reduce the Anxiety caused by Obsessions.
The Cycle of Obsession and Compulsion Consumes Time (often >1 hour/day) and Affects Normal Functioning.
Types of OCD-
- Contamination & Cleaning – fear of germs, repeated washing/cleaning.
- Checking – repeatedly checking locks, gas stoves, appliances.
- Symmetry & Ordering – arranging objects in a perfect or balanced way.
- Intrusive Thoughts – aggressive, sexual, or religious thoughts.
- Hoarding – difficulty discarding items, leading to clutter.
Etiology (Causes)-
OCD is multifactorial, involving:
- Biological factors:
-Imbalance in serotonin neurotransmission.
-Genetic predisposition (runs in families).
-Brain circuit abnormalities (orbitofrontal cortex, basal ganglia).
- Psychological factors:
-Perfectionistic or rigid personality traits.
-Negative thinking styles.
- Environmental factors:
-Childhood trauma, stress, or infections (PANDAS in children).
Clinical Features-
A condition in which frequent unwanted obsessions that cause you to perform compulsions-
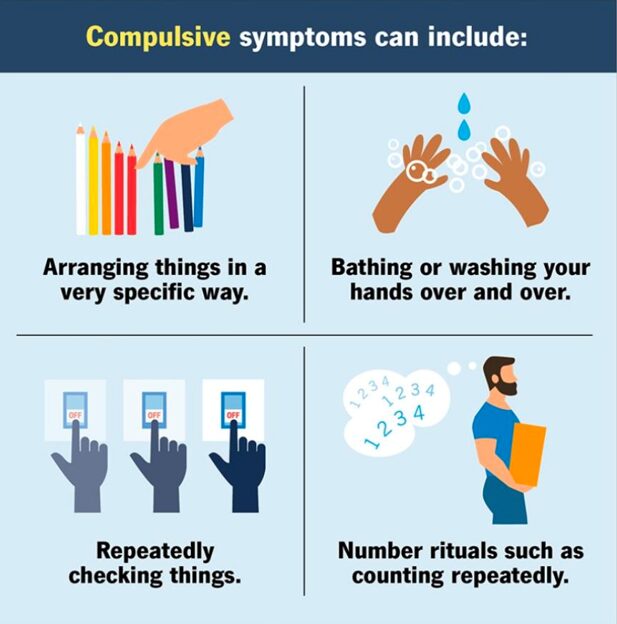
Obsessive symptoms can include-

Compulsive symptoms can include-

Diagnosis–
- Based on DSM-5 criteria → presence of obsessions, compulsions, or both, causing distress or impairment.
Tools–
-Yale-Brown Obsessive–Compulsive Scale (Y-BOCS).
-Structured psychiatric interviews.
Treatment-
Effective treatment often requires combined approaches:
- Psychotherapy
– Cognitive Behavioral Therapy (CBT), especially Exposure and Response Prevention (ERP).
– Helps break the obsession-compulsion cycle.
- Medications
-SSRIs (fluoxetine, sertraline, fluvoxamine).
-Clomipramine (a tricyclic antidepressant).
- Advanced Biological Therapies
-Deep Brain Stimulation (DBS).
-Transcranial Magnetic Stimulation (TMS).
Neuromodulation Treatment-
- Newest studies suggest Transcranial Magnetic stimulation (TMS)
– When combine with exposer and rituals prevention, it can be effective for OCD
-Uses magnetic field to stimulate Brain cells.
- Deep Brain stimulation( DBS)-
- Involves implanting a device in Brain.
- Has evidence of benefits but is invasive and complex.
Lifestyle & Support-
- Stress management- mindfulness, yoga, breathing, Regular exercise .
- Routine and structure- Daily schedule reduces uncertainty and compulsion.
- Limit trigger – Reduce unnecessary checking or Reassurance – seeking .
- Social support -Talk with friends , joint support group, Family education to reduce stigma and encourage treatment adherence.
- Digital Discipline – Limit excessive screening timing and Late Night Browsing and.
Complications-
- Severe Anxiety, Depression, or Suicidal Thoughts.
- Social Isolation and Relationship Problems.
- Work or Academic Decline.
- Poor Quality of Life due to time lost in Rituals.
Prognosis-
- With Treatment, 60–70% of Patients Show Improvement.
- Early Diagnosis and Adherence to Therapy Improve long-term Outcomes.
- Without Treatment, OCD can become Chronic and Disabling.
Deterrence & Patient Education-
- Most OCD Patients have insight (only 2–4% lack insight).
- Many Delay Treatment Until Symptoms are Severe.
- Since onset is often in Adolescence, Awareness should be Raised among Parents, Teachers, and Healthcare Workers for early Detection.
Enhancing Healthcare Team Outcomes-
- Interprofessional HealthCare Teamwork is key for effective OCD care.
- Roles: –
-Primary care → First contact, Referral.
-Psychiatrists → Diagnosis, Medications.
-Psychologists → Testing, CBT.
-Occupational Therapists → Daily living support.
-Social Workers → Connect to Resources.
-Pharmacists → ensure safe & effective medication use.
- Requires Good Communication, shared Decision-making, Ethics (Consent, Autonomy, Beneficence).
- Continuous Training keeps care Safe, Modern, and Patient-Centered.
Conclusion-
OCD is not a Habit but a Serious Mental Health Disorder that deserves Attention, Empathy, and Treatment. With Modern Therapies, Medications, and Support Systems, Recovery and Normal Living are possible. Awareness and Early Intervention can Break the Chains of Obsession and Compulsion, giving People Freedom from the invisible Prison of their Own Thoughts.
References-
1.American Psychiatric Association. DSM-5: Diagnostic and Statistical Manual of Mental Disorders (2013).
- WHO (2023). Obsessive–Compulsive Disorder Fact Sheet.
- Kaplan & Sadock’s Synopsis of Psychiatry.
4.Stein DJ, Costa DLC, Lochner C, Miguel EC, Reddy YCJ, Shavitt RG, van den Heuvel OA, Simpson HB. Obsessive-compulsive disorder. Nat Rev Dis Primers. 2019 Aug 01;5(1):52. [PMC free article] [PubMed]
5.Blanco-Vieira T, Radua J, Marcelino L, Bloch M, Mataix-Cols D, do Rosário MC. The genetic epidemiology of obsessive-compulsive disorder: a systematic review and meta-analysis. Transl Psychiatry. 2023 Jun 28;13(1):230. [PMC free article] [PubMed]
6.Mataix-Cols D, Rosario-Campos MC, Leckman JF. A multidimensional model of obsessive-compulsive disorder. Am J Psychiatry. 2005 Feb;162(2):228-38. [PubMed]
7.Bloch MH, Landeros-Weisenberger A, Rosario MC, Pittenger C, Leckman JF. Meta-analysis of the symptom structure of obsessive-compulsive disorder. Am J Psychiatry. 2008 Dec;165(12):1532-42. [PMC free article] [PubMed]
8.Taylor S, McKay D, Miguel EC, De Mathis MA, Andrade C, Ahuja N, Sookman D, Kwon JS, Huh MJ, Riemann BC, Cottraux J, O’Connor K, Hale LR, Abramowitz JS, Fontenelle LF, Storch EA. Musical obsessions: a comprehensive review of neglected clinical phenomena. J Anxiety Disord. 2014 Aug;28(6):580-9. [PubMed]